Federal regulators recently approved significant changes to how Tennessee’s Medicaid program operates and qualifies for federal funding. (1) (2) (3) The changes, officially known as TennCare III, have generated many questions, concerns, and misunderstandings. This list of FAQs attempts to provide clarity on the most common points of confusion. See TennCare III: Unpacking Tennessee’s New Medicaid “Block Grant” for a full analysis and additional details.
1. Does TennCare III replace unlimited federal Medicaid funding with a fixed or capped amount?
Tennessee’s federal Medicaid funding has been capped for over two decades and will remain capped under TennCare III. Since 1994, TennCare has operated with a waiver from certain federal rules. Longstanding federal administrative policy requires such waivers to be “budget neutral.” This means federal officials have capped our Medicaid funding at the amount they estimate they would have spent without the waiver. TennCare III will be subject to a similar – but less generous – budget neutrality cap based on specific enrollee groups (e.g. children, individuals with disabilities), per-person TennCare spending, expected Medicaid cost growth, and actual enrollment 1% above or below 2019 enrollment.
2. Is TennCare III a block grant?
No, not in the traditional sense. Under TennCare III, the federal government will continue to cover roughly 65% of all TennCare spending – up to a cap that will change each year based on national health care inflation projections and certain enrollment changes as noted above. A block grant, on the other hand, is usually a lump sum given to a state for some broad purpose. The full amount is available to states with few strings attached, and it is usually static from year-to-year unless Congress decides otherwise. The Community Development, Substance Abuse, and Mental Health Block Grants are all well-known, traditional block grants.
3. Is the new funding cap riskier than the old one?
Yes, but it’s unlikely that TennCare could have kept the old, more generous funding cap beyond June 2021. In fact, that is essentially what the state’s block grant proposal asked for – without success. TennCare’s per-enrollee spending and annual cost growth are lower than in most other Medicaid programs. As a result, the state’s longstanding funding cap never posed much financial risk to Tennessee. After TennCare’s 2016 waiver renewal, however, the Obama and Trump administrations changed how they would calculate states’ funding caps moving forward – based on federal watchdog concerns about overspending. (4) (5) (6) (7) (8) (9) As written, the changes would have held Tennessee to its own already low spending and cost trends – significantly reducing the state’s federal funding cap.
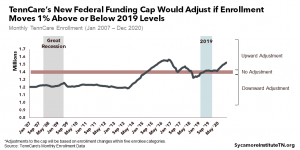
The TennCare III cap reflects some, but not all, of those changes – making it less risky than what federal officials might have required when TennCare II came up for renewal this summer. The most advantageous feature is that the TennCare III cap will grow based on national spending trends instead of Tennessee’s own recent trends (Figure 1). If the state does exceed its recalculated cap over the 10-year waiver period, it also has about $6 billion in cushion from the prior waiver that it can use to offset any overages.
Tennessee may also get up to 55% of the federal share of any difference between the cap and actual spending – without committing any additional state money. The actual amount will depend on if and how much Tennessee stays below the cap, along with the state’s performance on 10 to-be-determined quality metrics. State officials refer to this potential extra money as “shared savings.”
Figure 1
4. Can Tennessee use the shared savings dollars to pay for roads, education, etc.?
Yes and no. This new source of federal money can only pay for a handful of state-funded health programs, but it could free up state dollars to pay for other, unrestricted expenses. Existing state spending on a set of approved health programs would trigger a federal match of “shared savings” dollars (at Tennessee’s standard Medicaid match rate of about 65%). As a result, these matching funds could potentially free up as much as 65% of the state’s current spending on those health programs. While the waiver does not restrict how the state can use that freed-up money, TennCare and Governor Lee have said they intend to use it to improve the health of TennCare enrollees. (5)
Any new federal dollars from the TennCare III agreement will be non-recurring revenue, making it harder to predict. Tennessee does not have to draw down its federal “shared savings” dollars in the year they were earned, which gives policymakers some time to enter into any new obligations cautiously. Even so, health care spending can be unpredictable, and the federal funding caps that determine how much “shared savings” is available will reset to the state’s actual spending levels in five years. These trade-offs and limitations are likely to shape how policymakers use any freed-up state dollars.
5. Does TennCare III allow programs cuts with no oversight?
No. Any action to reduce eligibility or coverage standards below December 31, 2020 levels would be subject to all existing federal oversight and approval processes. Tennessee will still need prior federal approval for any program changes that would formally rollback an eligibility category or benefit.
6. Will coverage change for those who are already enrolled?
Maybe. TennCare III allows the state to restrict access to some prescription drugs through the use of a closed drug formulary, but other coverage changes will need federal approval. Enrollees could see changes to what drugs are covered, making this aspect of TennCare coverage more like private insurance and Medicare. TennCare III requires an exceptions process for people who need certain drugs that are not a covered, but the details have yet to be determined. All other changes to existing eligibility and benefits must go through the standard federal approval process.
The state can also make administrative changes without additional federal approval, which might affect enrollees in various ways. TennCare will be able to implement changes to enrollment processes, delivery systems, provider payments, and uncompensated care payments to hospitals at will – all of which could potentially affect current enrollees.
Figure 2
7. Where do the “savings” come from?
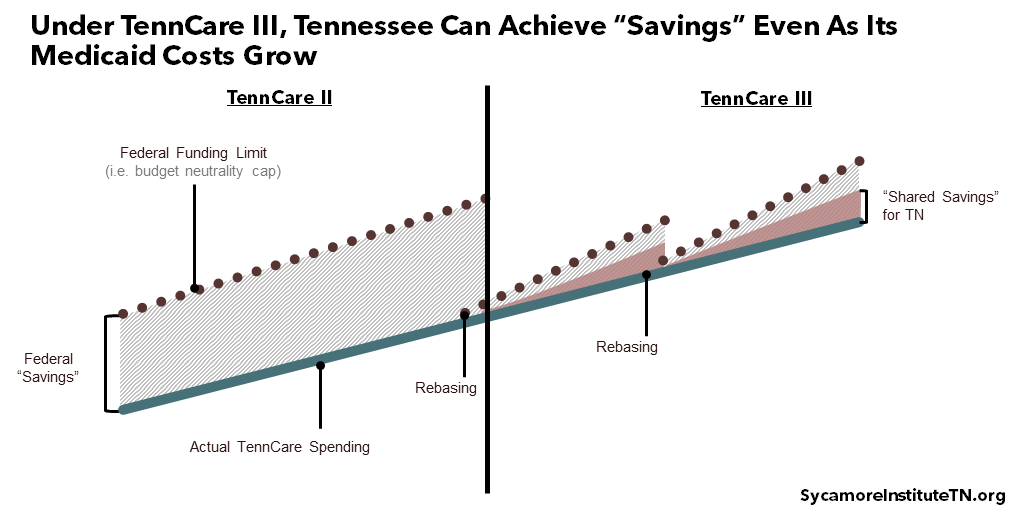
In a move that has led to much confusion, policymakers chose the word “savings” to describe extra federal funding that Tennessee would not otherwise receive. In the context of TennCare III, the word “savings” means the difference between TennCare’s actual spending and its federal funding cap. That cap is based on national Medicaid spending projections, which have generally been well above the state’s actual spending trends. If TennCare’s per-person spending grows slower than these national rates, Tennessee could get about half of the difference – officially known as “shared savings.” These savings can materialize even without any cuts to current spending (Figure 2).
TennCare could stay below its federal funding cap without program changes simply by maintaining past growth trends. The funding cap represents an estimate of what TennCare might cost the federal government if it did not have a waiver from traditional Medicaid rules. While not written in law, longstanding federal administrative policy requires waivers to be budget neutral so that federal spending does not rise faster than expected. For this reason, TennCare’s “budget neutrality cap” (aka the funding cap) does account for things like enrollment changes and rising health care costs.
The waiver also gives TennCare several new tools that it could use to constrain spending growth. These include a closed drug formulary and the ability to make changes at will to enrollment processes, delivery systems, provider payments, and uncompensated care payments to hospitals.
8. Does TennCare III jeopardize coverage for the 1.4 million enrollees currently on TennCare?
Current enrollees can expect changes to prescription drug coverage, but TennCare III does not pose any other new risks for current enrollees that did not already exist. The state has no additional incentive to reduce enrollment because the federal funding cap would also shrink by the same proportion. While the possibility of “shared savings” does give the state more short-term value from constraining per-person costs, the long-term value is now much less than before. Tennessee’s funding cap will be “rebased” in five years to its actual per-person costs, meaning a large drop in per-person spending would only generate extra federal funding for a limited time. Meanwhile, the state could face longer-term challenges when the cap is recalculated to reflect those lower costs.
9. Does TennCare III expand Medicaid?
No. TennCare III does not specifically advance or prevent Medicaid expansion. Under the new agreement, TennCare can expand eligibility to new groups without prior federal approval. However, it is unclear if TennCare III could generate enough new funding by itself to pay for hundreds of thousands of new enrollees. It will be hard to predict how much extra federal money Tennessee might qualify to get via “shared savings” in any particular year. And any such funding that does materialize will be non-recurring revenues, which are usually only used for one-time expenses. However, nothing in the TennCare III waiver precludes the state from separately seeking a broad eligibility expansion if policymakers choose to pursue that.
10. Is this a good or bad thing for Tennessee?
It could be both. Or neither. Frankly, we just don’t know yet. TennCare III’s impact on current enrollees, providers, and the state budget all depend on questions that have not yet been answered and decisions that have not yet been made. For example, can the state keep typical TennCare cost growth on the same, relatively low trajectory? How will policymakers use new flexibilities and freed-up state dollars? What will the drug formulary and the processes surrounding it look like? Until these questions are answered, the jury is out.
11. How will we know what the state is doing with its new flexibilities and shared savings?
Many of the changes that TennCare III could bring will remain subject to existing processes that unfold in the public eye. For example, all program changes must still meet existing notification and transparency requirements whether or not they need federal approval. Any state dollars freed up by new federal “shared savings” dollars will be allocated through the usual legislative process, and some aspects such as the intricacies of the new drug formulary could require a public rulemaking process.
However, transparency requirements are less clear for other administrative decisions and information. For example, 10 quality metrics must be picked to will help determine how much – if any – “shared savings” dollars the state could draw down. Tennessee must also develop implementation and evaluation plans that track how the state uses flexibilities within the waiver, as well as their impact. The public’s level of visibility into these types of decisions and the process policymakers will use to make them are both unclear.
12. Is this agreement legal?
We don’t know. Sycamore’s analysis of the TennCare III waiver focuses on what full implementation could mean for TennCare’s stakeholders, health in Tennessee, the state budget, and related public policy implications. We expect legal challenges at both the state and federal levels, and legal minds on both sides of this question have expressed confidence that their arguments will win out in court.
13. What happens if the Biden administration rescinds the agreement?
Tennessee and the Biden administration would negotiate a new waiver, which would likely entail more financial risk for the state than TennCare III. No matter what else happens, the previous TennCare waiver expires on June 30, 2021. After TennCare’s 2016 waiver renewal, the Obama and Trump administrations changed how they would calculate states’ funding caps moving forward – based on federal watchdog concerns about overspending. (4) (5) (6) (7) (8) (9) As written, the changes would have held Tennessee to its own already low spending and cost – significantly reducing the state’s federal funding cap. TennCare III’s cap includes some of the changes, but overall, the terms are more advantageous – even without the “shared savings” provision. Whether Tennessee could get the same deal (minus the “shared savings”) from the Biden administration is unclear.
The Biden administration could also use the negotiation as a bargaining chip to encourage Tennessee to expand Medicaid. During the state’s last renewal negotiation, for example, the Obama administration argued for changes to the state’s uncompensated care spending – contending that Medicaid expansion was a better way to fund care for the uninsured. (11) It is likely that the Biden administration would make similar efforts.
References
Click to Open/Close
- The Centers for Medicare & Medicaid Services (CMS) and TennCare. TennCare III: Tennessee’s 1115 Demonstration Waiver. [Online] January 8, 2021. https://www.tn.gov/content/dam/tn/tenncare/documents/tenncarewaiver.pdf.
- State of Tennessee. Tennessee Medicaid Block Grant Waiver Amendment Approved by Federal Government. [Online] January 8, 2021. https://www.tn.gov/governor/news/2021/1/8/tennessee-medicaid-block-grant-waiver-amendment-approved-by-federal-government.html.
- The Centers for Medicare & Medicaid Services (CMS). CMS Administrator Seema Verma’s Press Call Remarks as Prepared for Delivery on TennCare. [Online] January 8, 2021. https://www.cms.gov/newsroom/press-releases/cms-administrator-seema-vermas-press-call-remarks-prepared-delivery-tenncare.
- Hill, Timothy B. SMD # 18-009: Budget Neutrality Policies for Section 1115(a) Medicaid Demonstration Waivers. Centers for Medicare and Medicaid Services. [Online] August 22, 2018. https://www.medicaid.gov/Federal-Policy-Guidance/downloads/SMD18009.pdf.
- The Centers for Medicare & Medicaid Services (CMS). CMS Releases Formal Approach to Ensure Medicaid Demonstrations Remain Budget Neutral. [Online] August 22, 2018. https://www.cms.gov/newsroom/press-releases/cms-releases-formal-approach-ensure-medicaid-demonstrations-remain-budget-neutral.
- Karl, Anne. CMS Issues Additional Guidance on Budget Neutrality for Section 1115 Waivers. Manatt Health. [Online] August 24, 2018. Available from https://www.shvs.org/cms-issues-additional-guidance-on-budget-neutrality-for-section-1115-waivers/.
- U.S. Government Accountability Office (GAO). Medicaid Demonstrations: HHS’s Approval Process for Arkansas’s Medicaid Expansion Waiver Raises Cost Concerns. [Online] August 8, 2014. https://www.gao.gov/assets/670/665265.pdf.
- —. Medicaid Demonstrations: Federal Action Needed to Improve Oversight of Spending. [Online] April 2017. https://www.gao.gov/assets/690/683888.pdf.
- —. Medicaid Demonstration Waivers: Approval Process Raises Cost Concerns and Lacks Transparency. [Online] June 2013. https://www.gao.gov/assets/660/655483.pdf.
- TennCare. Quarterly Reports to the Centers for Medicare & Medicaid Services (CMS). [Online] 2013-2019. [Cited: January 12, 2020.] Available from https://www.medicaid.gov/medicaid/section-1115-demo/demonstration-and-waiver-list/83206.
- —. Tennessee Medicaid Block Grant Waiver Agreement: Frequently Asked Questions. [Online] January 8, 2020. https://www.tn.gov/content/dam/tn/tenncare/documents/TennCareBlockGrantFAQs.pdf.
- Galewitz, Phil. Tennessee, Kansas Also Get Warning: Expand Medicaid Or Risk Hospital Funds. Kaiser Health News. [Online] April 21, 2015. https://khn.org/news/tennessee-and-kansas-also-get-warning-expand-medicaid-or-risk-losing-hospital-funds/.